ECG Axis
Heart disease has become a significant medical concern in the US over the past several years and now accounts for around 800,000 deaths each year. The magnitude of this problem can be demonstrated by the fact that more people die from cardiac illness each year than from all forms of cancer combined. As the population grows and people retire, the use of procedures like electrocardiograms (ECG) to diagnose and treat heart conditions rises. Those planning to work in the cardiac industry should be familiar with aspects of evaluation like the ECG axis.
An Overview of the Electrocardiogram
The electrocardiogram is one of the most common noninvasive procedures used in cardiac care today to record the electrical activity of the heart. In most cases, a series of electrodes are placed on the patient’s chest and attached to a recording device. As electrical impulses travel through the heart, the electrodes pick up signals and transmit them to the computer for interpretation. The computer then produces either a printed or electronic tracing that is used by licensed providers to identify abnormalities in cardiac conduction or contraction. Additional information relating to EKG rhythms and interpretation can be reviewed in our previous posts.
Lead Placement and Electrical Conduction
The placement of the electrodes on the chest is strategically designed in order to produce different views of electrical activity. This allows medical personnel to identify problems and pinpoint the location where an abnormality is occurring. An ECG axis refers to the direction in which a wave of depolarization is travelling. It is important for impulses to move through the heart in a precise manner so that blood can be pumped efficiently. Cardiac illness can cause these signals to traverse the tissue in an abnormal manner and will usually result in a predictable pattern on the electrocardiogram. The ECG axis is one of the most important factors that physicians evaluate when diagnosing and treating patients. When an impulse is traveling toward an electrode it results in an upward deflection on the electrocardiograms while one moving away from an electrode causes a downward deflection.
Mean Vectors and Deviations
A normal mean electrical vector of the heart, in the frontal plane, is typically directed from the right shoulder toward the left leg because the signal originates in the right atrium and travels through the heart toward the left ventricle. Deviations between -30o and +90o are considered normal aberrations. When the left and right ventricles experience an increase in activity or bulk, the mean ECG axis will swing toward the abnormal ventricle. This action is referred to as a left or right deviation.
A left deviation between -30o and -90o may be a sign of an inferior myocardial infarction and possibly a left anterior fascicular block, but is sometimes considered normal in pregnancy or in patients suffering from emphysema. Other conditions that might cause a left deviation can include…
- Left bundle branch block
- Left ventricular hypertrophy
- Ventricular pacing
- Wolff-Parkinson-White Syndrome
The right deviation that falls between +90o and +180o may be a sign of a lateral myocardial infarction or left posterior fascicular block, but is often normal in children and dextrocardia. Other situations that could result in a right deviation include…
- Chronic obstructive pulmonary disease
- Right ventricular hypertrophy
- High levels of potassium
- Wolff-Parkinson-White Syndrome
Upper Left Quadrant Deviations
A deviation between that of +180o and -90o is known as an extreme shift and can result from ventricular rhythms, hyperkalemia, and more. Although it is helpful for technicians to understand the basics of the ECG axis, the evaluation and treatment of patients is outside their scope of practice and is the responsibility of licensed personnel such as a nurse and a physician. Those who have questions about the role of a technician within the cardiac care department are encouraged to speak with their employer to learn more about the position as well as avenues for advancement.
Isolating Cardiac Ischemia and Injury
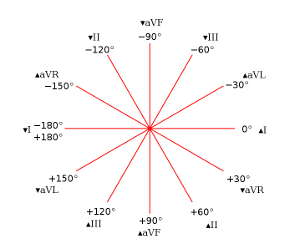 The twelve lead electrocardiogram is a very popular diagnostic option that is used within cardiovascular care because each lead offers a different and unique vantage point of the heart’s electrical activity. The ECG axis that is provided by each lead allows the physician to isolate ischemia and injury to a specific anatomical area of the heart. A widely used diagrammatic representation of the twelve vectors produced by this particular type of electrocardiogram is demonstrated using a hexaxial reference system to the right.
The twelve lead electrocardiogram is a very popular diagnostic option that is used within cardiovascular care because each lead offers a different and unique vantage point of the heart’s electrical activity. The ECG axis that is provided by each lead allows the physician to isolate ischemia and injury to a specific anatomical area of the heart. A widely used diagrammatic representation of the twelve vectors produced by this particular type of electrocardiogram is demonstrated using a hexaxial reference system to the right.
As shown by the system, leads II, III, and aVF have the inferior perspective of electrical activity; leads I, aVL, V5, and V6 provide the view from the lateral wall of the left ventricle; leads V1 and V2 show electrical activity as seen from the interventricular wall; and leads V3 and V4 offer the perspective from the anterior wall of the ventricles. Technicians should have a basic understanding of the ECG axis viewpoints that are produced by the 12 lead electrocardiogram, but are not usually required to perform the detailed analysis necessary to diagnose or treat patients. Additional details about lead placement can be found here.
Estimating the Mean Electrical Vector
There are a few approaches commonly used to estimate the mean electrical vector. One of the most popular ECG axis methods is to use leads I and aVF. 2 positives are considered normal while negatives show an extreme shift toward the upper left axis. A positive in lead I with a negative in aVF might indicate a left deviation while the reverse may mean a right deviation. Another quick method is to consider lead I and II together. A positive in both means that the vector lies between -30o and +90o. These two methods provide an estimate of the ECG axis.